Helicobacter pylori (H. pylori) is a common type of bacteria that can cause an infection in the lining of the stomach. Its importance remained unrecognised until 1982, when two Australian researchers, Dr Barry J Marshall and Dr J Robin Warren, a Fellow of the RCPA, discovered that the bacteria were almost always present in patients with gastritis.
At that time, it was generally believed that stress and lifestyle factors were the major causes of stomach infections, and it took until 1985 when Dr Marshall famously infected himself with the bacterium to prove it caused acute gastric illness. Since then, H. pylori has been widely recognised as a pathogenic organism that causes gastritis, peptic ulcer disease, and gastric cancer.
Now, more than 40 years later, H. pylori has attained ‘superbug status’, listed as a high priority organism by the World Health Organization for posing the greatest threat to human health due to its increasing antibiotic resistance. Dr Caitlin Keighley, microbiologist and infectious diseases physician, explains how a change in diagnostics can help guide treatment for patients.
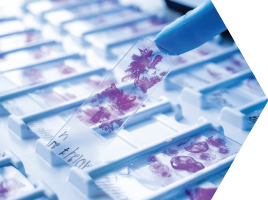
“An early advance in diagnosis was the move to detection using non-invasive specimens which require patients to give a blood, breath, or faeces sample. One of the most common methods is the urea breath test (UBT) which examines the breath for the presence of H. pylori. They are accurate tests that require patients to go to collection centres. We also use faecal antigen testing which detects active infection by identifying H. pylori specific antigens in a stool sample. This kind of sample is easy to get, anyone can do it without having to travel, and the test picks up current infection.
“Serology testing is also used for diagnosis but is not as accurate, especially in a low prevalence population. Serology can also remain positive for months to years after a patient has successfully cleared the infection. A positive result must therefore be confirmed by other methods,” said Dr Keighley.
Current guidelines recommend treating anyone diagnosed with H. pylori. Previously, there was a recommendation that asymptomatic individuals may not require treatment. No single drug cures H. pylori infection and most treatment regimens involve taking several medications for 7-14 days.
“Treatment for H. pylori is largely empiric and has quite a low success rate with increasing resistance to antibiotics. Primary treatment is esomeprazole, amoxicillin, clarithromycin; however, the Therapeutic Guidelines (eTG) success estimate of 85-90% is probably overestimated in current clinical practice.
“There have been focused efforts to tailor eradication therapy based on identifying genetic markers of resistance, which is an exciting advance. Being able to apply molecular markers of resistance to non-invasive samples would facilitate being able to skip some of that failure with first line therapy. We are on the cusp on the next era of development that will improve what we can do for H. pylori,” said Dr Keighley.